Pharmacogenetics in Primary Care: An Update
Advancements in the area of personalized medicine and understanding how one’s genetics affect health outcomes is an evolving science. The addition of pharmacogenetic testing to the armamentarium of primary care providers presents an opportunity to improve patient care.
AUTHOR
Karen L. Kier, PhD, MSc, RPh, BCPS, BCACP, CTTS, FASHP, FCCP, Professor of Pharmacy Practice; Director of Assessment; Director of Drug and Health Information; Preventive Care Specialist, ONU HealthWise; Raabe College of Pharmacy, Ohio Northern University, Ada, OH
PEER REVIEWER
Cynthia Sheppard Solomon, BSPharm, RPh, FASCP, CTTS, NCTTP, Clinical Assistant Professor, Department of Internal Medicine and Neurology, WSU-BSOM, Dayton, OH
EXECUTIVE SUMMARY
President Obama’s announcement in his 2015 State of the Union Address launched the Precision Medicine Initiative, a bold new research effort to revolutionize how we improve health and treat disease. Precision, or personalized, medicine focuses on identifying the unique patient factors that determine success in treatment while minimizing the risk of adverse reactions.
- One out of every five prescriptions written in the United States is for a medication that has actionable Food and Drug Administration labeling or evidence for pharmacogenomics.
- Each year, 125,000 hospital admissions are the result of adverse drug reactions (ADRs). The fear of ADRs and/or treatment failures can lead to the erosion of patient confidence in their physicians and may contribute to the attraction for alternative therapies.
- Pharmacogenetic biomarkers include genes that code for drug-metabolizing enzymes as well as those that code for transporter proteins. Pharmacodynamic biomarkers affect the action of drugs at the molecular level and are less well understood.
- Clinicians are provided helpful resources, such as the Dutch Pharmacogenomics Working Group (DPWG) and the Clinical Pharmacogenetics Implementation Consortium (CPIC). PharmGKB is a free online curator of information for actionable pharmacogenomics (PGx) recommendations.
- Because a patient’s genome does not change, testing for PGx typically is done once, and the results are available for improved drug selection over the course of a patient’s life. Barriers to more widespread use of PGx include the complexity of reporting, the variability in laboratory quality, and the challenges of third-party reimbursement.
Introduction
Advancing technology continues to challenge physicians in the practice of medicine. New research, techniques, medications, biologics, and other treatments can improve the prevention and management of disease. The advancements in the area of personalized medicine and understanding how one’s genetics affect health outcomes is an evolving science. In 2020 alone, 6,298 articles were indexed under the MESH heading of pharmacogenetics/pharmacogenomics by the National Library of Medicine.1 The abundance of literature and the potential for clinical implementation requires primary care providers (PCPs) to consult with a pharmacogenetics expert or team for better understanding of applying genetic testing as it relates to medications. It might surprise PCPs that one out of every five prescriptions written in the United States is for a medication that has actionable Food and Drug Administration (FDA) labeling or evidence for pharmacogenomics (PGx).2 A study by Van Driest et al found in a cohort of 10,000 patients that 91% had an actionable variant when genotyped for CYP2C19, CYP2C9, VKORC1, TPMT, and CYP3A5. The study also reported also that within the African American cohort, 96% had an actionable variant.3 A study of 52,942 subjects found that 65% were exposed to at least one PGx medication in the course of five years.2 These studies indicate that actionable PGx therapies are more common than one would realize. The addition of pharmacogenetic testing to the armamentarium of PCPs presents an opportunity to improve patient care.
Pharmacogenetics and pharmacogenomics are very similar terms that often are used interchangeably. Authors tend to use pharmacogenomics when discussing broader research about the relationship between the genome and pharmacotherapy, such as in genome-wide association studies (GWAS). Pharmacogenomics usually applies to a population. Pharmacogenetics more often is used when referring to specific genes and their influence on specific drugs. An example of this would be the study of how cytochrome P450 2C9 (CYP2C9) and VKORC1 polymorphisms affect warfarin pharmacokinetics and pharmacodynamics.4 Pharmacogenetics deals with individuals. See Table 1 for a glossary of terms.
Table 1. Glossary of Terms | ||
Term | Definition | Example |
Alleles Allele, variant | Variant form of a gene, one of two or more forms of a single gene | We inherit one allele from each parent. CYP2D6*2 would be one allele of the combined inherited genes. |
Star allele | A method to label haplotypes in genes | PharmVar Gene Expert Panels provide star determinations for variants in a gene. This label provides consistency in interpretation of gene pairs. |
Wild allele | Normal functioning allele; nonvariant allele | Two wild alleles indicate normal function and are displayed as *1/*1. |
Allele, loss of function | A mutation in which the altered gene lacks the molecular function of the wild-type gene | The loss of function (LOF) allele is considered recessive, so one usually results in an intermediate metabolizer and two LOF alleles usually result in a poor metabolizer. |
Diplotype | A specific combination of two haplotypes | A specific diplotype is one variant of all possible combinations of the haplotypes and is represented as a pair of star alleles, such as *1/*17. |
Haplotype | Set of DNA variations, or polymorphisms that tend to be inherited together | Variations in the DNA that are so close together that they tend not to recombine, and therefore tend to be passed down through the generations together. |
Polymorphism | Natural variation in a gene, DNA sequence, or chromosome | |
Single nucleotide polymorphism (SNP) | A genetic variant in which only one letter in the DNA sequence is changed. SNPs can be clinically relevant in changing risk of disease and drug effects. | SNPs represent one change in a DNA building block (nucleotide). An example could be a cystosine “C” is replaced with thymine “T.” |
Genotype | A particular DNA composition within a gene of interest | Eye color, where B is for brown eyes (dominant) and b is for blue eyes (recessive), so one’s genotype could be Bb. |
Phenotype | Physical characteristic expressed/observed with the given genotype | The genotype bb would be homozygous recessive and would be expressed as the phenotype of blue eyes. |
VKORC1 | Encodes for the enzyme vitamin K epoxide reductase complex subunit 1 | Enzymatic protein complex is responsible for reducing vitamin K 2,3-epoxide to its active form and affects warfarin anticoagulation. |
TMPT | Thiopurine methyltransferase or thiopurine S-methyltransferase is an enzyme that metabolizes drugs and serves as a pharmacogenomic biomarker. | TMPT is an essential enzyme in the metabolism of thiopurine drugs. |
CYP450 | A group of enzymes involved in drug metabolism and found in high levels in the liver | Ninety percent of drugs go through the CYP450 enzymes, with the highest percentage CYP3A4 and CYP2D6. |
DNA: Deoxyribonucleic acid | ||
Drug therapy or medication management is a fine balance between improving health outcomes and controlling chronic disease states while limiting adverse drug reactions. Many management recommendations are drawn from well-designed studies, but these focus on results in broad populations rather than individuals. Medications shown to be effective in these studies may be less effective in a particular patient, resulting in failure to reach the desired treatment goals. Ideally, therapy should see improved outcomes with acceptable therapeutic levels. Pharmacokinetics is one way that we can determine blood levels by determining drug elimination and the half-life of medication. However, pharmacokinetics does not always explain why patients handle drugs very differently with different outcomes. Pharmacogenetic studies and analysis are attempting to understand why drugs affect patients differently. With evidence, could a prescriber design drug therapy unique to a patient? The evidence provides some clues, but the science has more strides to make for better understanding of the dynamics of therapy.
Medications can cause unintended effects. Adverse drug reactions (ADRs) can be dangerous for patients and account for more than 3.5 million physician office visits each year with an estimated 1 million emergency department encounters. The U.S. Department of Health and Human Services (HHS) estimates that at least 125,000 hospital admissions each year are the result of ADRs. HHS estimates that ADRs prolong a hospital stay an average of 3.5 days.5
ADRs and/or treatment failure may erode patient confidence in their physician, or perhaps in the validity of the evidence used as a basis for their recommendation. This can lead to mistrust of pharmaceutical treatment as a whole and can reduce patient motivation to meet health management goals. This fear may contribute to the preference of some individuals for alternative therapies.
The emergence of PGx testing offers promise in mitigating some risks associated with medication therapy. Testing for known genetic variants that affect drug metabolism, receptor sensitivity, or drug transport potentially can enhance the therapeutic response to medication, reduce ADRs, and optimize treatment of disease. Although this can positively affect both disease-specific outcomes and patient satisfaction, PGx testing has its own complications. Testing may indicate that a commonly available medication is less advisable for a particular patient, but alternatives may not be readily accessible or considered first-line by payers. PGx testing facilities need to be certified to assure valid results, and many companies are marketing PGx testing directly to patients for both medications and potential disease-related genes. The physician needs to be assured that the results are from a legitimate laboratory. Many reports can be difficult to interpret regarding clinical application for the patient. Currently, many of the PGx testing panels are not covered by insurance companies or require prior authorization for testing. PGx testing has ethical issues that need to be considered and discussed with families prior to testing.6,7 The novelty of the technology may lead to patient uncertainty regarding the significance and implications of genetic testing results.
Pharmacogenetic Testing and Prescribing
Bridging the gap in provider understanding of PGx is essential to the future of primary care. PCPs are ideally positioned to counsel patients in a manner that will make this technology most clinically meaningful. PGx is an area where PCPs report a low index of confidence. In one national survey, the majority of PCPs reported that they do not feel well informed about PGx testing. Although more than half indicated that they received genetics training in medical school, most thought that the training was inadequate to prepare them to use PGx testing in their clinical decision-making. The lack of confidence in using PGx test results may be a reason why many PCPs responding to the survey reported that they have never ordered PGx testing.8 A multispecialty survey of U.S. physicians shows that primary care is not unique in this regard. With the sole exception of oncology specialists, the vast majority of physicians surveyed did not regularly order genetic testing, citing lack of information.9 A 2020 study of primary care and mental health providers found similar results when qualitative focus groups were conducted regarding pharmacogenetic testing for prescribing in depression. Several themes emerged from the research, including limited provider experience and knowledge, uncertainty of whether PGx would improve outcomes, misinterpretation of PGx results, and a concern of incorporating PGx testing into their workflow. The researchers noted that primary care providers felt less comfortable with PGx testing than psychiatric providers.10
Although PCPs indicate uncertainty about how to use PGx testing in clinical practice, there is broad acknowledgment of its potential utility. In the multispecialty survey, 97.6% of respondents indicated they believed that genetics may influence a patient’s response to drug therapies.9 In the PCP survey, almost two-thirds of respondents agreed that PGx testing represents a valuable potential tool to predict the risk of ADRs or the likelihood of efficacy. Among physicians who have used PGx testing, reducing drug toxicity and improving effectiveness were cited as significant observed benefits to patients.7 (See Table 2.)
Table 2. Goals of Pharmacogenetic Testing |
Some goals for pharmacogenetic testing include the following:
|
Principles of PGx
SNPs, Alleles, Genotypes, and Phenotypes
Different forms of genes that are passed on from parent to child are called alleles. The combination of alleles an individual inherits determines his or her genotype, and the expression of these alleles determines his or her phenotype. Genetic variation arises from the introduction of mutations, or alterations in the DNA sequence, in these alleles. The most commonly identified mutations are single nucleotide polymorphisms, also called SNPs. A particular SNP may or may not result in changes in protein regulation, expression, or activity.
When an identified SNP negatively affects protein function, it is termed a loss-of-function allele. Someone with one (heterozygote) or two (homozygote) loss-of-function alleles will have less overall protein expression and/or activity compared to someone with two normal-function alleles. When an SNP is identified that positively affects protein function, it is termed a gain-of-function allele. The presence of a gain-of-function allele, or duplication of a normal-function allele, may result in increased protein expression and/or enhanced activity. These genotypes can have a direct effect on numerous metabolic functions, including how individuals respond to certain drugs at a cellular level.
The nomenclature for two normal alleles is *1/*1 or is referred to as the wild type. A PGx testing result that indicates two active functioning alleles is the *1/*1 for any drug. Any number higher than 1 as a star allele, such as *2 or *17, indicates a change-in-function allele (either loss or increased activity). A patient with a PGx testing result of *1/*17 (two alleles are the diplotype) would have one active function allele and a change in function allele and would be heterozygous. A patient with test results of *17/*17 would be homozygous with two variant alleles. Some patients may have more than two alleles as a variant, such that one allele may have two or more copies. This would be denoted on a PGx testing result as *1/*17N or *1/*17x2. This seems fairly simple, but the interpretation can be difficult when applying it to drug therapy. Some variants are a loss-in-function while others are an increase-in-function allele. It is important look up the diplotypes for each drug because they can differ in response. Alleles also may result in altered response to medications because of abnormal binding at their site of action or receptors. These alleles may have different nomenclature than the traditional star (*) designations. For example, a PGx test report may indicate that a patient is HLA-B*58:01 positive for risk of allopurinol severe skin reactions.6 Websites such as PharmGKB and the Clinical Pharmacogenetics Implementation Consortium (CPIC) have reference charts to match the diplotype to the function. These websites will be discussed in more detail later in the article.
The effect that genetic variations have on drug metabolism is characterized by well-established phenotypes. A poor metabolizer is an individual with two inactive or loss-of-function alleles. In patients with this phenotype, drugs may not be metabolized efficiently. This can result in increased drug concentrations that can reach toxic levels. Ultrarapid metabolizers have gene duplicates and, therefore, increased drug metabolism. This can result in subtherapeutic drug levels at doses that likely would be effective in normal metabolizers. Figure 1 illustrates the consequences that these genetic variations can have on drug metabolism and, therefore, effectiveness and toxicity.11
Figure 1. Consequences of Genetic Variations on Drug Metabolism, Effectiveness, and Toxicity |
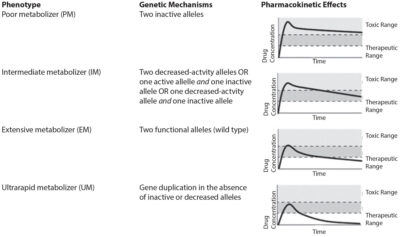 |
Reprinted with permission from Ravyn D, Ravyn V, Lowney R, Nasrallah HA. CYP450 pharmacogenetic treatment strategies for antipsychotics: A review of the evidence. Schizophr Res 2013;149:3. |
Types of PGx Biomarkers
The FDA refers to alleles that influence drug effectiveness and toxicity as “pharmacogenetic biomarkers.”12 PGx biomarkers are classified further as either pharmacokinetic (PK) or pharmacodynamic (PD). PK biomarkers affect how the body absorbs, distributes, metabolizes, and excretes drugs. Their effects on drug bioavailability, blood concentrations, and distribution into tissues are easy to measure and, therefore, they are well understood and studied.13 This class of biomarkers includes genes that code for drug-metabolizing enzymes, such as CYP2D6, CYP2C9, and CYP2C19. Also included are genes that code for transporter proteins, such as OAT1B1 and P-glycoprotein. Drug-metabolizing enzymes, such as the cytochrome P450s, biotransform drugs into metabolites more readily eliminated by the body or modified by other enzymes.14 Transporters function to move drugs in and out of cells and across barriers such as the small intestine, liver, kidney, and brain. For this reason, they sometimes are referred to as “gatekeepers.”15 They also are involved in directly eliminating drugs via biliary and urinary excretion. Two important biomarkers involved in drug transport include SLCO1B1, which codes for the OAT1B1 transporter, and ABCB1, sometimes called the “multidrug resistance gene,” which codes for P-glycoprotein.16 OAT1B1 is an influx transporter, meaning it moves drugs into cells. P-glycoprotein is an efflux transporter, meaning it moves drugs out of cells and into the intestinal tract, bile, blood, or urine.17
PD biomarkers are less well understood. These biomarkers affect the action of drugs at the molecular level. Their effects are harder to isolate and measure, and uncertainty of the exact mechanism of action for many drugs further limits research in this area. Just as there are different subtypes of PK biomarkers, there also are subtypes of PD biomarkers. Some effect drug response directly, whereas others may play a more indirect role as a result of a genetic variance that affects the underlying disease process. Indirect PD biomarkers still may significantly influence the efficacy, toxicity, and/or laboratory values of treatment. An example of a direct effect would be opioid binding to the mu-opioid receptor. Genetic variations of the OPRM1 gene, which codes for the mu-opioid receptor, may affect the amount of pain attenuation achieved with opioids.13 An example of an indirect PD biomarker would be HLA-B*15:02, which is strongly associated with carbamazepine use and the risk of Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), despite it not being involved in the drug’s known mechanism of action.17 Apolipoprotein E (APOE) is an example of a PD biomarker that is associated with laboratory values. Certain variations in APOE are associated with greater low-density lipoprotein (LDL) reductions in patients being treated for high cholesterol.18
Although PGx biomarkers can increase the physician’s knowledge of how patients potentially will respond to medications, some PK biomarkers may affect the metabolism of a drug in a manner that does not result in a PD difference, either good or bad. A list of significant PGx biomarkers can be found on the FDA website.12 Tables 3 and 4 describe some of the important PK and PD biomarkers.
Table 3. Examples of Pharmacokinetic Biomarkers | |||
Biomarker | Phenotype | Affected Drug | Effects and Considerations |
CYP2D6 | Poor metabolizer Ultrarapid metabolizer | Atomoxetine Metoprolol Nortriptyline | AUC (area under the curve) increased up to 900% compared to normal metabolizers. Product insert specifies a more conservative dosing regimen for this phenotype.44 Plasma concentrations increased up to 390% and heart rate and blood pressure significantly decreased compared to other phenotypes.45 AUC decreased by 35% in patients with three active alleles and 80% in patients with 13 active alleles compared to normal metabolizers.46 A dose increase of up to 150% has been recommended.46 |
CYP2C9 | Poor metabolizer | Celecoxib | AUC increased up to 600% compared to normal metabolizers.47 Product insert recommends a 50% decreased maintenance dose and to avoid in individuals with juvenile rheumatoid arthritis.48 |
CYP2C19 | Poor metabolizer Ultrarapid metabolizer | Clopidogrel Citalopram Omeprazole | AUC of active metabolite decreased 65% compared to normal metabolizers.49 A meta-analysis showed a 55% increase in cardiovascular events, myocardial infarction, or stroke in individuals with this phenotype compared to normal metabolizers undergoing percutaneous coronary intervention for acute coronary syndrome.50 Product insert recommends using an alternative platelet inhibitor.51 AUC increased 107% compared to normal metabolizers. Product insert recommends 20 mg maximum daily dose in individuals with this phenotype.52 AUC decreased 52% compared to normal metabolizers.53 Dose increases up to 300% have been recommended.46 |
UGT1A1 | Poor metabolizer | Ezetimibe | AUC increased 177% compared to normal metabolizers.54 |
UGT2B15 | Poor metabolizer | Lorazepam | AUC increased 72% compared to normal metabolizers.55 |
ABCB1 (P-glycoprotein) | 2677TT/3435TT | Amlodipine | AUC decreased 33% in 2677TT/3435TT homozygotes compared to 2677GG/3435CC homozygotes.56 |
SLCO1B1 (OAT1B1) | Poor transporter (c.521CC genotype) | Atorvastatin | AUC increased 145% compared to c.521TT homozygotes.57 Similar results have been observed in other studies.58,59 The maximum recommended dose is 20 mg daily in individuals with this phenotype.60 |
Disclaimer: Evidence may exist that conflicts with the examples used in this table. | |||
Table 4. Examples of Pharmacodynamic Biomarkers | |
Biomarkers | Effects |
Beta-1 adrenergic receptor (ADRB1) | Metoprolol-induced decrease in diastolic blood pressure was significantly greater in individuals with the 389Arg/Arg genotype compared to those with the Arg/Gly and Gly/Gly genotype.61 |
Beta-2 adrenergic receptor (ADRB2) | Albuterol resistance was more likely in GLY allele carriers.62 |
Factor II | Factor II 20210A allele carriers taking estrogen-containing oral contraceptive (OC) |
Factor V Leiden | Odds ratios ranging from 11-41 have been reported for combination of Factor V Leiden allele and OC use.66 |
HLA-B*1502 | HLA-B*1502 is associated with increased risk of Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) in Asians taking carbamazepine.67,68 |
Opioid receptor mu-1 (OPRM1) | Oxycodone-induced pain attenuation was decreased in OPRM1 118G allele carriers. These individuals required increased oxycodone doses compared to 118AA homozygotes.69 |
Platelet endothelial aggregation receptor-1 (PEAR1) | rs12041331 A allele carriers receiving aspirin had significantly increased risk of myocardial infarction compared with GG homozygotes.70 |
Potassium voltage-gated channel (KCNH2, hERG) | QTc interval is prolonged 14 ms per KCNH2 897Lys allele in patients receiving steady state methadone compared to non-allele carriers.71 |
Serotonin transporter (5HTT/SLC6A4) | Caucasians with the 5HTT L/L or L/S genotypes had increased response to selective serotonin reuptake inhibitor therapy compared to individuals with the S/S genotype.72 |
VKORC1 | VKORC1 AA and GG homozygotes may have up to a 100% difference in warfarin dose requirements.73 |
Disclaimer: Evidence may exist that conflicts with the examples used in this table. | |
Several resources are available to help with understanding the clinical utility of actionable PGx testing. The websites are updated frequently as new evidence emerges. The FDA recognizes the importance of pharmacogenomics in the drug development process and the ability to apply this research to design new drugs. The FDA’s Genomics and Targeted Therapy Group is part of the Office of Clinical Pharmacology and is tasked with ensuring that PGx strategies are part of all phases of drug development. Their core functions involve regulatory review, research, policy development, education, and outreach.19 The FDA provides guidance for PGx with the medication approval labeling and maintains the Table of Pharmacogenomic Biomarkers in Drug Labeling.12 The table includes the generic name of the drug, the therapeutic area, the biomarkers, and the labeling section where the information can be found. A detailed version that includes the labeling text is available to download. As of December 2020, the table has 433 entries of medications that have PGx incorporated into the labeling. Not all of the entries are unique because some medications have multiple biomarkers that are affected and have duplicate entries. When sorting the data by therapeutic use, the leading field of PGx medication labeling is oncology, with 103 unique drug entities. Some of the other therapeutic use areas include psychiatry with 35 unique entries, infectious disease with 29, neurology with 27, cardiology with 16, and anesthesiology/pain management with 16.12 Within this list, the FDA has identified 47 drugs with evidence for PGx therapeutic recommendations and 16 drugs where PGx gene-drug pairs have an effect on safety or response to therapy.
The Table of Pharmacogenetic Association is provided by the FDA as a quick and easy reference for those gene-drug interactions that the FDA states have “sufficient scientific evidence to suggest that subgroups of patients with certain genetic variants, or genetic variant-inferred phenotypes, are likely to have altered drug metabolism … differential therapeutic effects, including differences in risks of adverse events.” With this table, the FDA makes an important distinction that they are not suggesting or advocating for routine PGx testing unless it is a common diagnostic test.20
With 433 labeling entries by the FDA, one might wonder how many of these would be considered actionable or have an effect on therapeutic recommendations? This is where other resources come into the picture to help provide the clinician with information to guide evidence-based recommendations. The two most recognized expert groups are the Dutch Pharmacogenomics Working Group (DPWG) and the Clinical Pharmacogenetics Implementation Consortium (CPIC). Consideration should be given to national professional organization guidelines, such as the American College of Rheumatology, which updated the gout guidelines in 2020 with expanded information on HLA-B*58:01 testing prior to allopurinol initiation in patients.21 The Pharmacogenomics Knowledge Base, known as PharmGKB, is a free online curator of information from multiple sources and is a good resource to check for actionable PGx recommendations (www.pharmgkb.org).22 PharmGKB provides a webpage, Very Important Pharmacogenes, that provides a detailed list of the gene-drug interactions or genes with tumor pharmacogenomics. In June 2020, the list was divided into Tier 1, Tier 2, and cancer genome to reflect the strength of evidence. Thirty-four pharmacogenes made Tier 1 for strong evidence for recommendations to manage patients with PGx testing.23
PharmGKB includes breaking news related to PGx testing and evidence. For example, they have started a webpage on PGx testing information that is relevant to COVID-19 treatments. There is emerging evidence that the patient’s response to COVID-19 therapies may be correlated to their genome and its variants.24 Some early data express some concern for drug-gene interactions, with drugs such as hydroxychloroquine, chloroquine, azithromycin, remdesivir, corticosteroids, and lopinavir/ritonavir.25
There are 123 drugs in PharmGKB’s Clinical Guideline Annotations section, with 71 recommendations from CPIC and 95 from DPWG. If the clinician goes to the website and selects tramadol, one would see that DPWG has guidelines from 2018 but CPIC does not have one listed. Currently, CPIC is working on an updated opioid PGx statement, including tramadol, that should be released in 2021. The DPWG recommendations are for CYP2D6 and its clinical effect on pain management in poor, intermediate, and ultrarapid metabolizers.26
Warfarin is an interesting example within PharmGKB, since it links to the CPIC guideline (https://cpicpgx.org/content/guideline/publication/warfarin/2017/28198005.pdf).27 When the link is selected, the CPIC expert group provides a clinical PGx dosing algorithm for warfarin within the document’s Figure 2. It shows the difference in PGx testing of alleles based on patient ancestry. The algorithm is based on knowing VKORC1 and CYP2C9 *2 and *3 genotypes. If the patient is of non-African ancestry, then it provides strong evidence for PGx dosing. However, if the patient self-reports African ancestry, then it is important to note that PGx algorithm dosing should be done only if the additional CYP2C9 alleles of *5, *6, *8, and *11 were tested. If these were not included in the testing, then the patient should be dosed clinically without PGx data. This is an excellent example of how ancestry can affect the variants that need to be tested.
If a standard panel of VKORC1 and CYP2C9 *2 and *3 had been ordered without the additional *5, *6, *8, and *11 genotypes in a patient with African ancestry, the results would provide no more additional data than dosing without the PGx testing.4,27,28 Studies have shown that the use of the PGx dosing algorithm has better outcomes than traditional dosing strategies. Getting the right PGx data is essential for better clinical outcomes with less bleeding.29,30
Of the actionable drug-gene pair associations, two-thirds of these pairs are drug metabolizing enzyme genes, and about 80% of them are encoded in the cytochrome P450 enzymes. A small number are associated with transporter genes, with the majority encoded by the human leukocyte antigen (HLA) genes.
Table 5 shows some of the more common drug-gene pair associations that would be encountered within primary care practice.7,12
Table 5. Pharmacogenomics for Common Drugs | |||
Drug | Gene | Guidelines | Actionable Group |
Allopurinol | HLA-B | CPIC, FDA | Yes |
Amitriptyline | CYP2D6 | CPIC, FDA | Yes |
Aripiprazole | CYP2D6 | DPWG, FDA | Yes |
Atorvastatin | SLCO1B1 | CPIC, DPWG, FDA | No |
Azithromycin | ABCB1 | No | No |
Carbamazepine | HLA-A/HLA-B | CPIC | Yes |
Carvedilol | CYP2D6 | DPWG | Yes |
Celecoxib | CYP2C9 | CPIC | Yes |
Citalopram | CYP2C19 | CPIC, DPWG, FDA | Yes |
Clopidogrel | CYP2C19 | CPIC, DPWG, FDA | Yes |
Codeine | CYP2D6 | CPIC, DPWG, FDA | Yes |
Dexlansoprazole | CYP2C19 | CPIC | Yes |
Diazepam | CYP2C19 | FDA | Yes |
Escitalopram | CYP2C19 | CPIC, DPWG, FDA | Yes |
Esomeprazole | CYP2C19 | CPIC, DPWG | Yes |
Omeprazole | CYP2C19 | CPIC, DPWG | Yes |
Ondansetron | CYP2D6 | CPIC | No |
Oxcarbazepine | HLA-B | CPIC, FDA | Yes |
Pantoprazole | CYP2C19 | CPIC, DPWG, FDA | Yes |
Paroxetine | CYP2D6 | CPIC, DPWG | No |
Risperidone | CYP2D6 | CPIC, DPWG | No |
Rosuvastatin | SLCO1B1 | FDA | Yes |
Sertraline | CYP2C19 | CPIC, DPWG, FDA | Yes |
Simvastatin | SLCO1B1 | CPIC, DPWG | Yes |
Tolterodine | CYP2D6 | FDA | Yes |
Tramadol | CYP2D6 | DPWG, FDA | Yes |
Venlafaxine | CYP2D6 | CPIC, DPWG, FDA | Yes |
Voriconazole | CYP2C19 | CPIC, DPWG, FDA | Yes |
Warfarin | CYP2C9/VKORC1 | CPIC, DPWG, FDA | Yes |
National Institutes of Health Initiative
The National Human Genome Research Institute of the National Institutes of Health (NIH) has developed a consortium to enhance the use of genomic medicine. The initiative is for Implementing Genomics into Practice (IGNITE). The project funds research to incorporate genomic information into clinical care. In addition, the funding can be used to explore methods for effective implementation, diffusion, and sustainability in diverse clinical settings. Two of the funding divisions are the Science and Effectiveness of Medicine as well as Electronic Medical Records and Genomics Network (eMERGE). These divisions are working to find ways to get genomic information that improves clinical outcomes in health records so that practitioners have access to vital PGx testing information. The IGNITE program’s website will provide valuable information as funded projects are completed.31
PGx Testing Issues
Some significant barriers exist pertaining to ordering and receiving PGx testing. The ideal situation would be preemptive testing, easily accessible in an electronic health record, that prompts the prescriber before initiating a drug with actionable PGx. Naturally, the patient would respond with no side effect. In addition, the patient would understand why PGx testing is necessary and would consent to testing by a certified Clinical Laboratory Improvements Amendments (CLIA) laboratory. A 2017 study evaluated laboratories that performed CYP2D6 and CYP2C19 testing and found significant variations. Not only the reports but also the testing panels and unique alleles were different. The number of alleles ranged from 15 to 21 for both genes, with a turnaround time of anywhere from one to two days to four to six weeks. It is hard to do preemptive testing, let alone reactive testing, for a new medication when results come back a month later. In addition, the labs were not consistent in which alleles were tested, making therapeutic decisions difficult. Some labs offered different interpretations for the same genotype to phenotype translation.32 With direct-to-consumer (DTC) PGx testing, the clinician often is bypassed when results are sent to the patient. Educating patients to understand why sharing this information with a provider could be important in managing medications is vital. This could be a new screening question when taking a patient history. Sometimes, even sharing family PGx data can be helpful as well.33 A study found that 69% of patients would be willing to share their results with a healthcare professional.34
PCPs need to be aware that, when patients select their own labs, those labs may not meet the CLIA accreditation standards. The data may not be helpful to the prescriber or a prescriber could question the validity of the results. Patients will respond to DTC labs that have the best marketing ploy vs. looking for a CLIA lab unless they are educated about the importance of CLIA. A prescriber should look for a CLIA-certified lab when ordering PGx testing. Results from a CLIA-certified laboratory should include analytic validity, clinical validity, and clinical utility while maintaining ethical, legal, and social implications. Analytic validity is the ability to measure the genotype of interest both accurately and reliably. Clinical validity is the ability of the test to detect or predict the phenotype associated with the genotype. Clinical utility indicates that measuring the PGx matters and will be useful in managing a patient’s medications. This is why the CPIC guidelines indicate when a PGx test has strong evidence for clinical utility. Physicians can verify if a lab is CLIA certified, but it can be hard to find if the PGx will be covered by insurance and, ultimately, which panel actually is covered. Many combination panels may not be covered by insurance compared to single panels. Providers should encourage patients to use the blood sample methods vs. saliva. Both are accurate when done appropriately, but so many factors can alter a saliva test when patients do not follow the directions. A provider also should consider if the lab provides interpretations of the lab results in a clinically useful report and if they offer a consulting service with a PGx expert. Some institutions have CLIA-certified PGx labs with a PGx consult service.35
Other factors to consider are whether the testing will be covered by third-party payers or whether patients will be willing to pay out-of-pocket expenses. Some payers will cover only single panel tests, not comprehensive testing. A recent meta-analysis evaluated the clinical utility of combinatorial panels for drug selection in major depressive disorder (MDD). The combinatorial panels include gene families that would be essential for antidepressant prescribing as well as combining tests for both pharmacokinetic and pharmacodynamics genes. The combinatorial panels showed a statistically significant improvement when compared to unguided care in both response and remission of MDD.36 An advantage of a combinatorial panel is having the multiple tests for a drug, such as citalopram, which is metabolized by CYP2C19 to an active metabolite that is then further metabolized by CYP2D6 before being eliminated. A single CYP2C19 panel would have missed this additional CYP enzyme step in the metabolism process.37
Several medications have different PGx testing requirements based on ancestry history. Many times, this information is self-reported, and clinicians need to rely on that history to order the correct allele variant panels. The previous example with warfarin illustrates this problem. In addition, patient self-reporting often is inaccurate, and they might not be aware of ancestry history.38
Applied PGx
To illustrate how PGx information can affect pharmaceutical management in clinical practice, an illustration drawn from a class of medications that is both commonly used and significantly affected by known biomarkers may be useful. Consider the following hypothetical cases.
Case 1: Depression
T.J. is a 21-year-old Caucasian male with MDD that has not been well controlled. His current medication is paroxetine 20 mg daily for eight weeks. He expresses “a little” improvement in his depression. This is his second trial of antidepressants. He had a six-week trial of fluvoxamine 50 mg daily. He did not like the sertraline because he “just didn’t feel right.” He reports a family history of depression and anxiety but does not know what medications his mother took. He does not smoke, but occasionally drinks alcohol on the weekends. His Patient Health Questionnaire-9 (PHQ-9) was 21 (severe) prior to initiation of paroxetine. His current PHQ-9 score is 18 (moderately severe). All labs are within normal limits. Would T.J. be a good candidate for PGx testing?
Yes, T.J. would be a good candidate because he has failed two different therapies. He continues to have high PHQ-9 scores, showing lack of response to medications, and he may be having some side effects. It is difficult to know if they are side effects without asking additional questions. Other common side effects to selective serotonin reuptake inhibitors (SSRIs) should be discussed with the patient to see if he can describe in better detail what he means by “just didn’t feel right.” Another good thing to assess prior to considering failure of therapy because of potential genetic variance would be patient adherence to the medication regimens. Did the patient stop the medication because of not feeling right? Did the patient not have an adequate trial of either medication? Adherence is a vital component of managing patients and an important part of interviewing/history.
Do paroxetine and fluvoxamine have a similar CYP450 metabolism?
Yes, both drugs go through the CYP2D6 pathway for metabolism. This would provide further justification for doing genetic testing. This clue helps in deciding what panels could be helpful for this patient. So, CYP2D6 would be important, as well as CYP2C19, because if we select a different SSRI pathway, then we may consider CYP2C19 pending genetic testing. Some providers might have a good justification for starting a CYP2C19 agent prior to genetic testing or if the panels would not be covered by payers.
You order PGx testing, and the following results are available: CYP1A2: *1/*1; CYP2B6: *1/*1; CYP2C19: *1/*1; CYP2D6: *1/*2x2; CYP3A5: *1/*1; HLA-B*15:02: negative; HLA-A*31:01: negative; SCLO1B1: *1/*1.
In using the CPIC Guidelines for SSRI Medications (https://cpicpgx.org/content/guideline/publication/SSRI/2015/25974703.pdf), it would be useful to know the status of the genetic results.36 A table of assignments of likely phenotypes based on diplotypes is provided in the CPIC guidelines. Based on Table 1a CYP2D6, T.J. would be an ultrarapid metabolizer. The CYP2D6 *1/*2x2 means that there are three alleles, and this provides an activity score of 3 and the classification of ultrarapid metabolizer. This would help to explain why two different CYP2D6 metabolized drugs did not improve T.J.’s depression. The blood levels would be subtherapeutic at therapeutic dosing of both paroxetine and fluvoxamine. Both of these drugs are addressed in the CPIC guidelines. CPIC has a strong recommendation to use an alternative option other than paroxetine in an ultrarapid metabolizer. CPIC has no recommendation for agent suggestion with fluvoxamine because of lack of evidence.
Based on CPIC, an alternative antidepressant that does not depend on the CYP2D6 system would be preferred. Looking at the CYP2C19 testing, the CPIC Table 1b indicates that the *1/*1 phenotype would be considered an extensive metabolizer (normal dosing). This is a great example of why you look up the phenotype with the guidelines — they can have different classifications. In this case, it does not change the recommendation. The CPIC guidelines offer two choices for an extensive metabolizer. These choices are citalopram/escitalopram at normal dosing or sertraline at normal dosing. Something to consider when choosing between these therapies is the that citalopram/escitalopram has a second metabolism that goes through the CYP2D6 pathway. Both still are options because the second metabolite does not contribute much to the overall antidepressant effects. However, the choice of sertraline still would be acceptable, since the majority of the drug goes through the CYP2C19 pathway. The CPIC guidelines rate the evidence for these two choices as strong. Clearly, these are not the only antidepressants on the market, but they are the ones that have been evaluated with evidence from CPIC. CPIC also has guidelines for the tricyclic antidepressants but have not provided guidelines for the serotonin-norepinephrine reuptake inhibitor class of antidepressants.
Case 2: Gout
M.P. is a 77-year-old Asian male who recently was diagnosed with gout. The patient has had two gout attacks confirmed in the last six months. Each time the patient had severe stomach pain and nausea with ibuprofen 800 mg three times daily despite taking it with meals. The patient had guaiac-positive stools both times and had to be converted to colchicine to manage the attacks. The patient was started on a short-term proton pump inhibitor to manage the gastrointestinal (GI) distress. As the prescriber, you want to start allopurinol for gout prophylaxis. The patient takes no other medications and has no other disease states. He exercises every day with tai chi. He does not drink alcohol, smoke, or use illicit substances. He does use some traditional Chinese herbs. In contacting the pharmacist to evaluate, they determine them to be more nutritional and vitamin-based. He takes one supplement that contains green tea and ginseng.
What is M.P.’s risk for a GI bleed? His risk factors include age, ibuprofen use, gout diagnosis, and herbal supplement ginseng.39 Could PGx testing provide insight into the GI bleed with ibuprofen?
Yes, PGx testing could provide some insight for nonsteroidal anti-inflammatory drugs (NSAIDs). CPIC has guidelines for NSAIDs. In the guidelines, you will see that poor metabolizers are at an increased risk of adverse effects, in particular those patients with a CYP2C9 of *2/*3 and *3/*3 phenotype. Ibuprofen is called out specifically because it has a linkage disequilibrium with CYP2C8 *3/*3 phenotype. Linkage disequilibrium occurs when a nonrandom link or association of two alleles occurs at two or more locations within the genetic code. Haplotypes will not occur at the usual frequency when the alleles are linked.6
The CPIC guidelines recommend an alternative NSAID if these phenotypes are present. Other alternatives suggested are sulindac, naproxen, aspirin, and ketorolac. The best therapeutic option, based on evidence, in treating gout would be naproxen. The patient did respond to colchicine and is awaiting prophylaxis treatment. An open-label pragmatic trial found naproxen and low-dose colchicine to be equivalent in managing gout flares, but patients had slightly more diarrhea with colchicine.40 (CPIC Guidelines for NSAIDs:41 https://cpicpgx.org/content/guideline/publication/NSAID/2020/32189324.pdf.)
What are the major risk factors for developing skin reactions to allopurinol in this patient? Asian ancestry is the biggest factor. More investigation needs to determine if M.P. is of Han-Chinese descent. The CPIC guideline for allopurinol provides a table with the frequency of HLA-B*58:01 with allopurinol-induced severe skin reactions. The highest prevalence is in Han-Chinese. After exploring the ancestry, you find out that M.P. is from Taiwan and is Han-Chinese.
Is this patient a good candidate for PGx testing? Because of M.P.’s Han-Chinese ancestry, the recommendation is to test for HLA-B*58:01. If testing is not available, then avoid the use of allopurinol. The FDA labeling is consistent with the CPIC guidelines.42
You order PGx testing and the following results are available: CYP1A2: *1/*1; CYP2B6: *1/*1; CYP2C19: *1/*1; CYP2C8: *3/*3; CYP2C9: *3/*3; CYP2D6: *1/*1; CYP3A5: *1/*1; HLA-B*15:02: negative; HLA-A*31:01: negative; HLA-B*58:01: positive; SCLO1B1: *1/*1.
Using the CPIC Guidelines for Allopurinol42 (https://cpicpgx.org/content/guideline/publication/allopurinol/2013/23232549.pdf), and with the HLA-B*58:01 positive test, allopurinol is contraindicated with a strong CPIC recommendation. Febuxostat would be a safer alternative for prophylaxis.43
Summary
Increased knowledge in the area of genomic sciences is likely to have an expanding effect on medical care as more evidence is attained with more funding to improve the science. Projects like IGNITE offer continued research into application-based PGx testing that can improve clinical outcomes. Improving the evidence and science can help improve acceptance by payers, patients, and other practitioners. PGx recommendations can be accessed from FDA labeling and PharmGKB, as well as the CPIC guidelines.
It is critical that physicians, particularly PCPs, seek to assume a leadership role in the implementation of genomic science in patient care. Ongoing education will help them use this information to manage medications and high-risk conditions optimally. The development of coordinated care models, such as accountable care organizations and the patient-centered medical home, also will leverage the skill sets of a broader segment of the healthcare team and greatly benefit the implementation of this technology.
Despite significant barriers, creating evidence-based protocols for implementation will yield optimal results for physicians and patients as genetic information takes a more prominent place in patient care. PCPs must become part of the development of these protocols for this technology to yield the greatest potential benefits.
Editor’s note: Portions of this article appeared in “The Future: Pharmacogenetics in Primary Care”by Elizabeth Black, MD; Brian T. Hocum, PharmD, CGP; and Kevin J. Black, MAT, published in the October 2014 issue of Primary Care Reports.
References
A complete list of references is available online: http://bit.ly/390O8Zx